A small compilation of nurse anesthesia care plans
These anesthesia care plans are meant to inspire nurse anesthesia residents when they are making their care plans. Always make sure you fully understand and "own" your care plan. Your plan must be specific for your patient and should always be with the most up-to-date information.
Larynx and Laryngeal Nerve Injury
Anatomy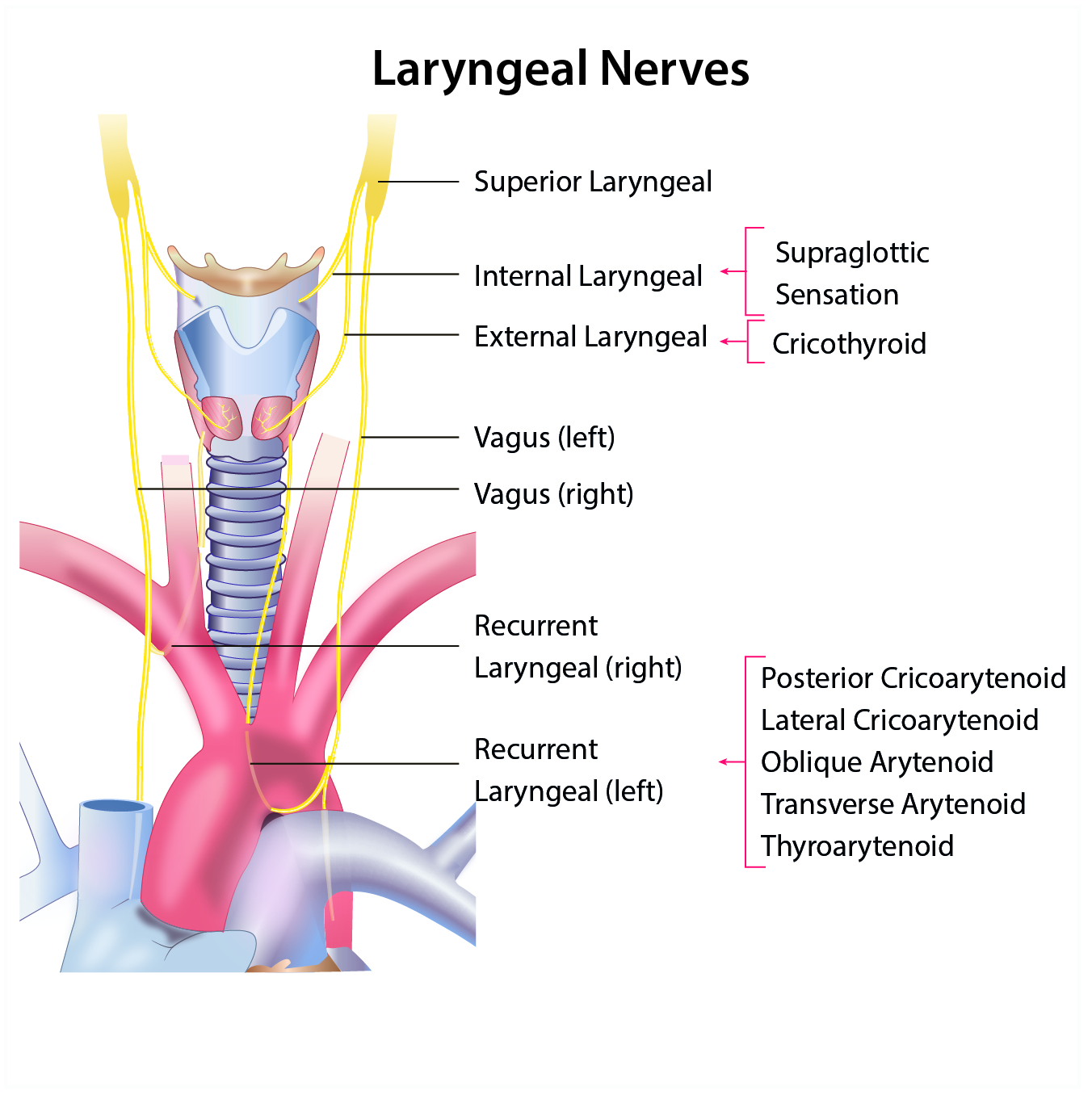
The larynx is located at the level of C-3 to C-6 and supports the hyoid bone
- 3 paired cartilages
- Arytenoids, corniculates, and cuneiforms
- 3 unpaired cartilages
- Epiglottis, thyroid, cricoid
- Trachea C-6 to T-4, T-5
- The Vagus nerve - CN X
- It provides sensation to the airway below the epiglottis and divides into
Superior laryngeal nerve
- External(motor) nerve, which innervates the cricothyroid muscle
- Internal (sensory) nerve to the larynx between the epiglottis and the vocal cords
Recurrent laryngeal nerve
- Innervates muscles of the larynx and trachea except the cricothyroid muscle
- RLN around the right subclavian vein
- LLN around the aorta
- Vocal cord movement
- Posterior cricoarytenoid muscle abducts vocal cords
- The lateral cricoarytenoid muscle adducts vocal cords
IX - The glossopharyngeal nerve supplies sensation to the tongue, tonsils, and soft palate
Laryngeal nerve injury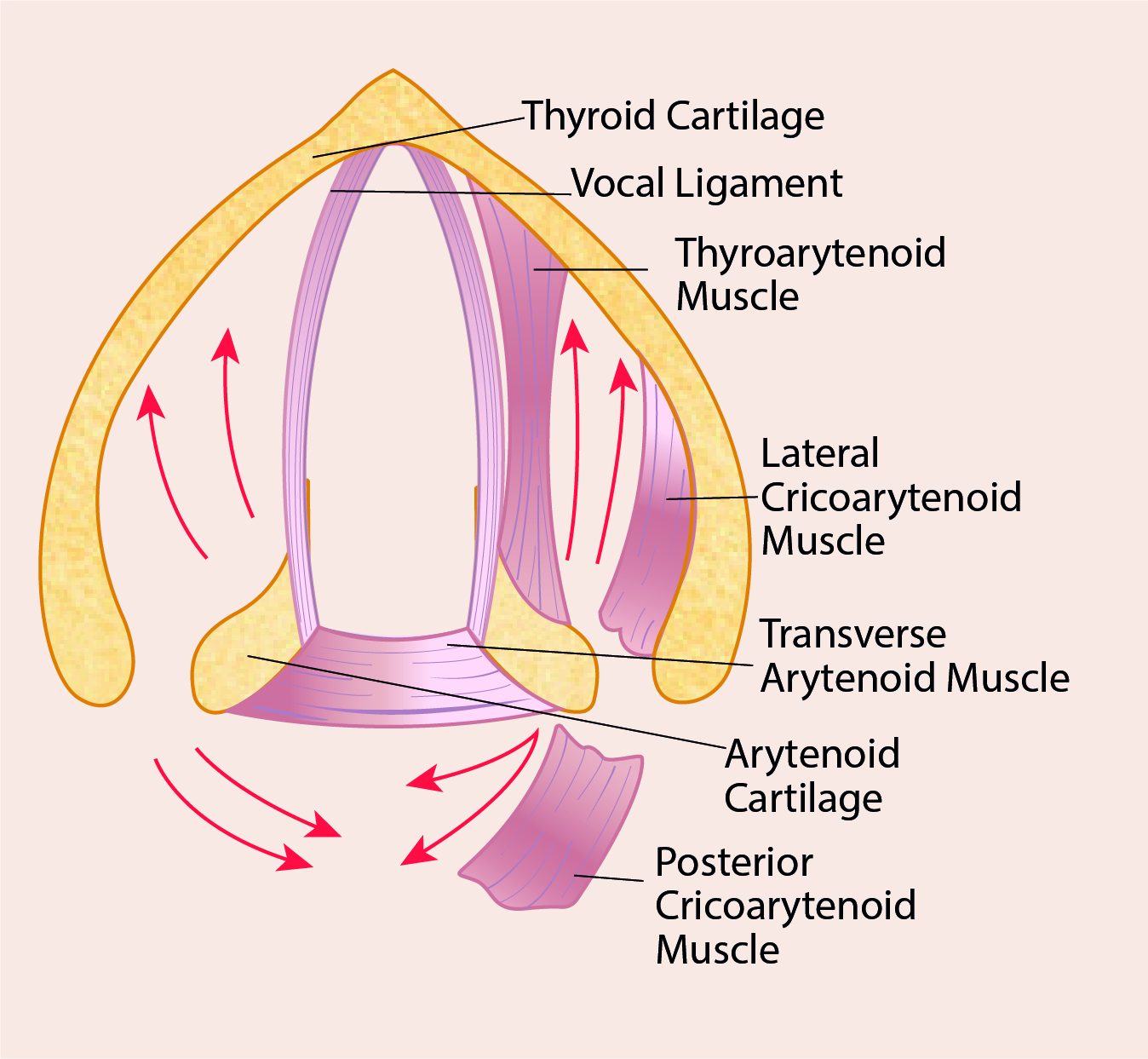
Superior laryngeal nerve
- Unilateral - minimal effects
- Bilateral - hoarseness
Recurrent laryngeal nerve - watch the cords move post-thyroidectomy
- Unilateral - hoarseness
- Bilateral
- Acute causes stridor, respiratory distress
- Chronic causes aphonia
Vagus nerve
- Unilateral causes hoarseness
- Bilateral causes aphonia - have pt phonate "e"