A small compilation of nurse anesthesia care plans
These anesthesia care plans are meant to inspire nurse anesthesia residents when they are making their care plans. Always make sure you fully understand and "own" your care plan. Your plan must be specific for your patient and should always be with the most up-to-date information.
Myringotomy and Tube Placement
 The myringotomy and tube, or M and T, patients are mostly young and have a history of recurrent otitis media, manifested by fluid in the middle ear, which is defined as six or more episodes in the prior year.
The myringotomy and tube, or M and T, patients are mostly young and have a history of recurrent otitis media, manifested by fluid in the middle ear, which is defined as six or more episodes in the prior year.
Untreated otitis media may permanently damage the middle ear and cause hearing loss. Children often have accompanying recurrent upper respiratory infections, which usually resolve with M and T.
Procedure
Surgery
Usually short, may not require IV, and can be done with mask GA
Position
Supine with head turned to the surgeon
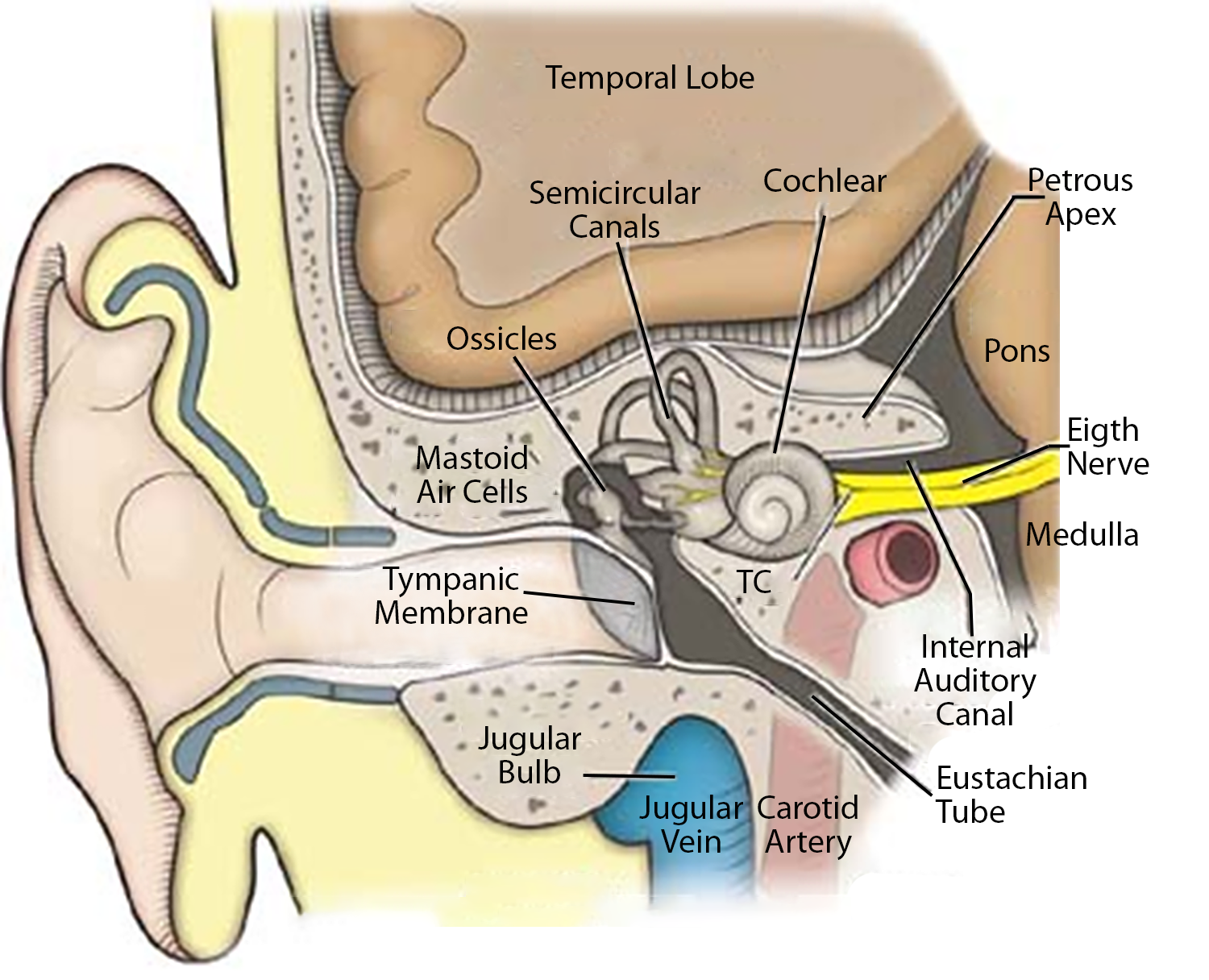
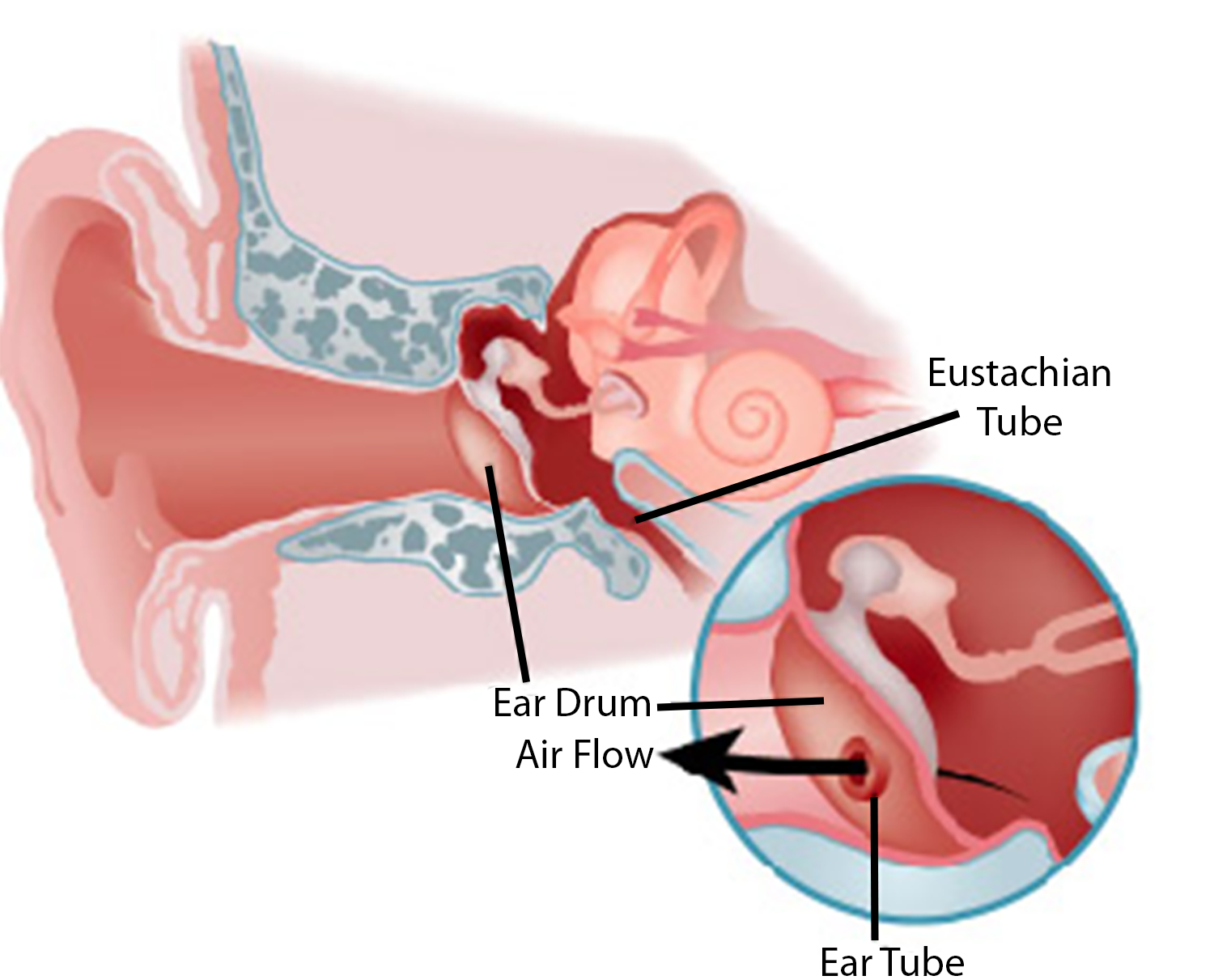 Hold the head still during Myringotomy! Ear speculum is placed in the ear, cerumen is removed, and an incision is made in the tympanic membrane. The tube is then placed in a straddling position over the tympanic membrane. Antibiotic and steroid eardrops are frequently inserted into the external auditory canal.
Hold the head still during Myringotomy! Ear speculum is placed in the ear, cerumen is removed, and an incision is made in the tympanic membrane. The tube is then placed in a straddling position over the tympanic membrane. Antibiotic and steroid eardrops are frequently inserted into the external auditory canal.
Morbidity
Infection, hearing loss, vertigo, facial nerve dysfunction, spinal fluid leak.
Anesthesia considerations
Avoid the use of N2O due to it being 34x more soluble than nitrogen and, therefore, will accumulate in closed spaces and increase the risk of creating pressure in the middle ear. The tube in place may not be clinically relevant to reduce this pressure
Hold head still during surgery
Volatile agent off when starting the second ear
Risk of airway obstruction
Use a precordial stethoscope