A small compilation of nurse anesthesia care plans
These anesthesia care plans are meant to inspire nurse anesthesia residents when they are making their care plans. Always make sure you fully understand and "own" your care plan. Your plan must be specific for your patient and should always be with the most up-to-date information.
Renal Fistula / AV Graft
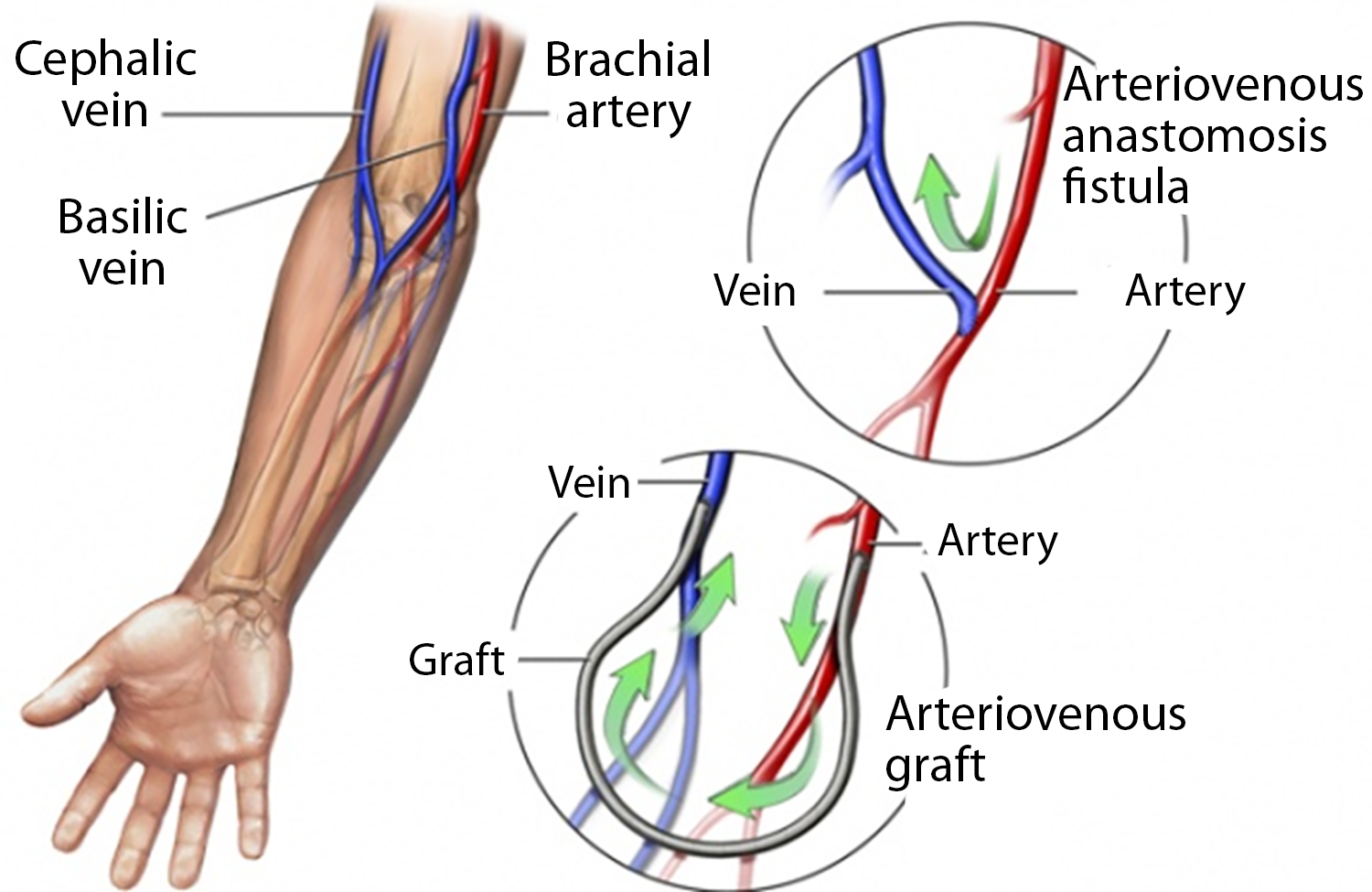 The autogenous AV fistula is the current procedure of choice for patients requiring permanent hemodialysis access. Blood flow in the autogenous AV fistula increases with time, and the resulting vein wall thickening prevents venous tears and infiltration during dialysis. The standard AV fistula is usually constructed by anastomosing the cephalic vein to the radial artery at the wrist level. Access can also be built in the upper arm as a straight communication between the brachial artery above the elbow and the basilic or axillary vein. A Doppler flow probe may be used.
The autogenous AV fistula is the current procedure of choice for patients requiring permanent hemodialysis access. Blood flow in the autogenous AV fistula increases with time, and the resulting vein wall thickening prevents venous tears and infiltration during dialysis. The standard AV fistula is usually constructed by anastomosing the cephalic vein to the radial artery at the wrist level. Access can also be built in the upper arm as a straight communication between the brachial artery above the elbow and the basilic or axillary vein. A Doppler flow probe may be used.
AV Fistulas
Connection of artery to superficial vein
Lowest complication rate
Long-lasting
Require 6-12 weeks for maturation
- Avoid BP or sticks on the chosen arm
AV Grafts
A graft made of synthetic material connects the artery and a large, deep vein.
Can be used 2-4 weeks post surgery
Shorter life than fistulas
- Prone to infection, may require declotting
Anesthetic Considerations:
Consider interscalene block
- Note coagulation status if on dialysis
The patient still needs pain medication during the procedure
Keep BP within 20% of baseline to ensure graft perfusion - some use pressors, some fluids
Antibiotics with graft placement
- Cefazolin 1 g
Respiratory
Pulmonary edema due to fluid overload
Hemodialysis contributes to hypoxemia due to V/Q mismatch and hypoventilation
Cardiac
HTN related to fluid overload
Renal
Access weights and thus the effect of dialysis
Note K+-level if using succinylcholine
Hematologic
Chronic anemia due to bone marrow depression, lack of erythropoietin, nutritional deficiency, and diminished red-cell survival
Patients adjust via increased CO2 and increased 2,3-DPG
- The right shift in the oxygen dissociation curve enables O2 unloading
GI
NV, anorexia, decreased gastric emptying
- Consider premedication with Reglan and Ranitidine
Neuro
Neuropathies
Pain with tunneling of graft